


Stomach
Following the oral cavity, the bolus is swallowed, passes through the esophagus via peristalsis, and reaches the stomach. The stomach is subdivided into the fundus, acting as the food reservoir where the ingested bolus remains until it reaches the distal stomach, whose function is to mix, grind and sieve the contents allowing only chyme to pass the pyloric sphincter. As food enters the proximal stomach, mechanosensitive receptor cell sense distension stimulating the release of gastrin from endocrine cells, which act on parietal cells to release HCl. The bolus is the rounded mass obtained before swallowing the chewed, lubricated food. In the distal stomach, antral contraction waves (ACW) mix the bolus with gastric fluid, and the shear forces generated by ACW, combined with HCl, break the physical structures remaining in the bolus. Gastric secretions in the fed and fasted state vary from < 1 ml/min to >10 ml/min and a total of 2-3 L/day containing mostly water, HCl, mucus, enzymes, and intrinsic factor. Under fasted conditions, the typical pH of the stomach is between 1.5 – 2; immediately following consumption, the pH increases between 4 – 6 due to the buffering capacity of the food materials contained in the bolus; within 1 hr, sufficient acid is secreted to decrease the pH <3.
Antral Contraction Waves
Reticulated antral waves occur in both the fasted and fed states, originating at the top of the antrum and propagating toward the pyloric sphincter. Under fasted conditions, contractions are weak and infrequent, while, in the fed state, weak and shallow tonic contracts move food from the fundus to the antrum, where strong, longitudinal contractions force the bolus and gastric fluid toward the pyloric sphincter and, upon retropulsion, generate significant shear forces to break down macrostructural elements of the bolus. Antral wave contractions do not occur in isolation, as 2-3 contractions occur at a rate of ~3 cycles/min. As peristaltic waves reach the pylorus sphincter, the width increases and indentations deepen, forcing the content against the narrowed sphincter resulting in fluid flow in the opposite direction (retropulsion), where the most significant shear forces are generated. The pyloric sphincter restricts the particle size in the chyme or the acidic aqueous dispersion of food particles entering the first segment of the small intestinal, the duodenum, to less than 1-2 mm while the larger particles remain and additional AWC further mixing and disintegrates particles.
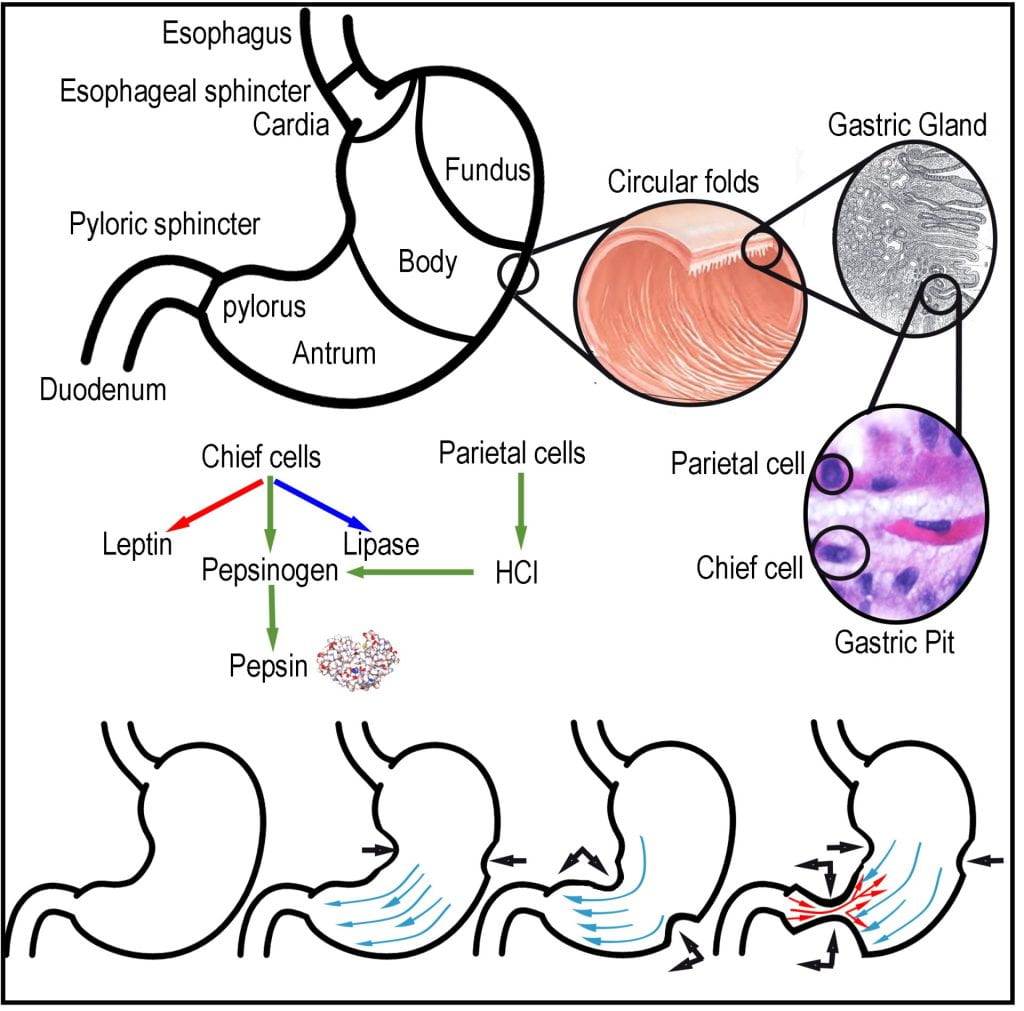
Gastric Enzymes

The cephalic response triggers endocrine cells in the stomach to release gastrin starting a cascade that acts on chief and parietal cells to release the inactive zymogen (pepsinogen) and HCl, respectively. Upon mixing the gastric fluid is acidified and protease enzymes are activated (pepsin) to begin digestion. As part of the cephalic response, salivary secretions increase via conditioned reflexes. Decreased pH is important in the stomach as it drops to 1.5, killing most bacteria, denaturing food proteins, causing them to unfold, and increasing their surface area for digestive enzymes to access.
Chief cells located in the gastric pits of the stomach lining secrete the inactive zymogen pepsinogen and, when exposed to the hydrochloric acid excreted from the parietal cells, is converted to the active enzyme pepsin. In the case of proteases, to prevent self-digestion, inactive forms of the enzyme, zymogens, are produced that require an alteration in the structure before they can become catalytic enzymes. Unlike other human digestive enzymes, pepsin’s optimal activity occurs pH 1.5-2.0 compared to most other digestive enzymes with an optimal pH ~ 7. Pepsin is an endopeptidase that cleaves proteins in the middle liberating two smaller peptides but not individual amino acids. Gastric lipase is an acid-stable enzyme that does not require bile or co-lipase and preferentially cleaves short and long-chain triglycerides at the SN1 or SN3 positions, generating one free fatty acid and either 1,2- or 2, 3-diacylglycerol. Although not an enzyme, the intrinsic factor is a glycoprotein that binds vitamin B12, allowing its absorption at the terminal ileum.
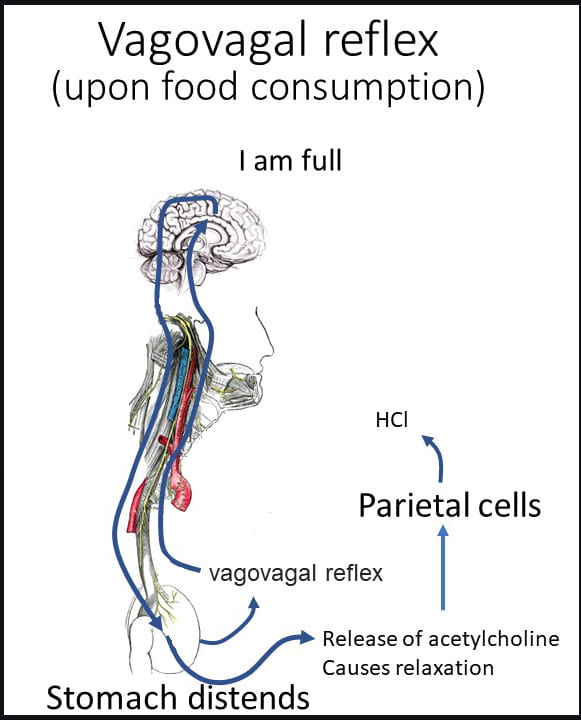
Vagovagal Reflex
Upon food consumption, the gastric cavity expands, distension initiates the vagovagal reflex. The vagovagal reflex communicates fullness via mechanosensitive and other vagal afferents, which are the neuronal component of the gut–brain axis allowing information to flow from the GI and viscera to the central nervous system. Distension triggers the release of acetylcholine causing the relaxation of muscles along the gastrointestinal tract allowing for further distension and additional acid production in the stomach. The reflex is the first cue to initiate satiation, the short-term drive to stop eating, or your perception of fullness.
Intrinsic Factor
Intrinsic factor, or cobalamin binding intrinsic factor, is a glycoprotein secreted in the gastric compartment by the parietal cells and is required to absorb the essential vitamin B12 at the distal ileum. A lack of intrinsic factors results in a B12 deficiency impairing the development of red blood cells resulting in pernicious anemia.